Hysterectomy (removal of the uterus)
What is a hysterectomy? How should you prepare for your operation? Below, you can read about the procedure, the related risks and the post-operative period following a hysterectomy.

Removal of female genitals
You may wish to have your female genitals fully or partially removed. For example, because you are experiencing dysphoria or because you want to undergo masculinising genital surgery (with urethral extension). The image below shows an overview of the female genitals.
Partially or fully removing your female genitals will have a direct impact on your fertility and any possibility of having biological children.
You can have multiple female genitalia removed. The various gynaecological operations are listed below:
- Removal of the uterus (hysterectomy)
- Removal of the vagina (colpectomy)
- Removal of the ovaries (oophorectomy)
- Removal of the fallopian tubes (salpingectomy )
These procedures can be conducted in various combinations. In addition, all of them can be combined with the removal of the breasts (mastectomy).
The various operations and combinations have different effects on your endocrine system, fertility and desire to have your own, biological children. It is therefore important that you carefully consider which organs you would like to have removed and what a logical combination would be for you. Discuss this with your gynaecologist. If you wish to have metoidioplasty or phalloplasty without urethral extension, then, in principle, there is no need for you to have the female genitals removed. If you do wish to have the urethral extension procedure, however, then it is necessary to have the female genitals removed.


About the hysterectomy
A hysterectomy is an operation by which your uterus will be removed. The reason for removal may, for example, be because you suffer from what is known as ‘abnormal uterine bleeding’, or you are experiencing gender dysphoria in relation to the uterus, or with a view to genital surgery. During the removal of the uterus, the fallopian tubes are removed at the same time; these are attached to the uterus. This will not affect your fertility, as the ovaries can remain in place, if you so wish.
More information about the preparations and reimbursement of operation costs can be found here.
The operation
The uterus can be removed in two ways:
- Keyhole surgery (laparoscopy): to remove only the uterus (and the ovaries), or in combination with a mastectomy.
- Robotic laparoscopic surgery: combination of removal of uterus and vagina. This procedure is conducted by the Da Vinci robot and leaves fewer scars than the keyhole surgery.
Keyhole surgery (laparoscopy)
Keyhole surgery is used when only the uterus (and not the vagina) is removed, or the uterus is removed in combination with the ovaries and/or breasts.
At the beginning of the procedure, a catheter will be inserted under general anaesthesia into your urethra to drain urine. Following this technique, the gynaecologist will make three to four incisions in the abdominal wall (see Figure 1). Through an incision just below the navel, a viewing tube will be inserted into the abdomen; the other incisions are intended to insert instruments into the abdominal cavity to detach the uterus and possibly the ovaries. At the end of the operation, the uterus is removed through the vagina.
With keyhole surgery, there is always a small risk that, during the procedure, the gynaecologist will need to perform abdominal surgery through a vertical or horizontal incision.

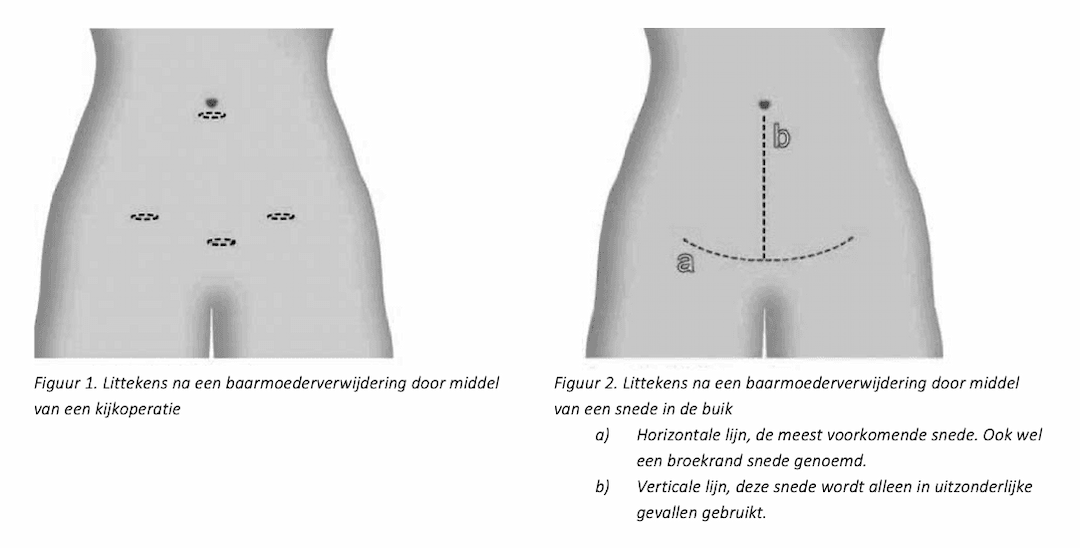
Figure 1) Keyhole surgery (laparoscopy)
Hysterectomy in combination with other gynaecological operations
A hysterectomy is often combined with another gynaecological operation. The advantages of this are that you only need to be anaesthetised once and will have only one recovery period. Combined operations are:
- Hysterectomy and oophorectomy (removal of the ovaries)
- Hysterectomy and mastectomy (removal of the breasts)
- Hysterectomy and colpectomy (removal of the vagina)
Combination 1: Hysterectomy and oophorectomy (removal of the ovaries)
In combination with a hysterectomy, you may opt to have your ovaries removed at the same time. As this also means that you will be infertile after the operation, you need to think about whether or not you would like to have a biological child in the future. More information about fertility is available here and on the following page (disclaimer: only available in Dutch) you can find more information about fertility preservation regarding to different genital surgeries.
It is important to realize that once your ovaries have been removed, you will no longer be able to produce your own sex hormones. This means you will need hormone therapy for the rest of your life. Some people choose to keep their ovaries as a 'backup' for hormone therapy. It is also possible to keep the ovaries and have only the fallopian tubes removed. This is considered a "low-complexity surgery". It is used when there is a strong desire to prevent pregnancy.
The same surgical technique is used as that for a hysterectomy alone. The procedure takes the same amount of time and involves the same risks and recovery time.
Combination 2: Hysterectomy and mastectomy (removal of the breasts)
Removal of the uterus may be combined with removal of the breasts (subcutaneous mastectomy). The ovaries can also be removed (this means that you will be infertile after the operation, which is why you should think about whether or not you would like to have biological children in the future). More information about fertility is available here and on the following page (disclaimer: only available in Dutch) you can find more information about fertility preservation regarding to different genital surgeries.
This combined operation is performed jointly by a plastic surgeon and a gynaecologist. The length of the recovery period will not be longer for these combined procedures.
Combination 3: Hysterectomy and colpectomy (removal of the vagina)
Removal of the uterus can be combined with removal of the vagina (colpectomy). In this combination, it is possible to remove the vagina and uterus via robotic surgery. This procedure can also be combined with the removal of the ovaries.
It is not possible to combine removal of vagina, uterus and breasts in one operation, as this would take too long. More information about this surgery is explained here.

Aftercare
You will need to stay in bed for 3 days after the operation. The catheter will usually be removed in the operating theatre and you should be able to urinate normally within a few hours. After urinating, your bladder will be scanned to make sure it is empty. If your bladder is not empty enough, the catheter will be replaced and will be removed again after about a week.
After a hysterectomy, urinary problems, such as difficulty to hold urine, can sometimes occur. This is because, during the operation, the bladder has been detached from the uterus. These urinary problems almost always go away by themselves, over time.
It is often advised to wait until the wounds are completely closed before swimming, taking a bath or going to the sauna. This often takes 4 to 6 weeks. This is to prevent the stitches from dissolving too early and you getting infections in the wound. Brief showers are allowed. You are not allowed to exercise or lift heavy objects for six weeks, as this may cause bleeding or the build-up of excessive fluid.
Medication and pain relief
You can discuss the continuation and use of medication with your physician. As soon as you are able to get out of bed, the thrombosis injections are no longer necessary. You may be prescribed a course of antibiotics for the first week after surgery to reduce the risk of infection. You can take painkillers in the form of paracetamol and diclofenac.
Complications and risks during and after surgery
With a single hysterectomy, the risk of complications is low. If the hysterectomy is combined with colpectomy, the risk of complications increases by around 20%. This increase is due to the removal of the vagina, which is a complex procedure. Most of these complications are mild, but some can be serious. Below is a list of possible complications that may occur before or after the operation.
- Haemorrhaging during or after surgery. Loss of blood and fluids during the operation is common, but if there is a large amount of blood loss, this is considered a complication. A blood transfusion may then be necessary. Haemorrhaging may also occur after the operation (including once your are back home again), and may require another operation to stop the bleeding. Sometimes, it is necessary to insert a gauze to stop the bleeding.
- Infection. The abdominal incisions or those in the vagina can become infected. This can already occur in the hospital. Sometimes, it can be treated with antibiotics, but in other instances, surgery will be needed to clear up the infection.
- Thrombosis. With any operation, there is a slightly increased risk of thrombosis (i.e. a blood clot in a blood vessel). You can reduce the risk of this happening by starting to move around again as soon as you can, after the operation, rather than lying still in bed. In hospital, you will also be provided with medication that will help to prevent this.
- Damage to bladder, bowel or urinary tract. During the operation, the bladder, bowel or urinary tract may become damaged. If this is obvious during the operation, it will be repaired immediately, if possible. Sometimes, a separate operation will be needed. If the bladder is damaged, a urinary catheter will be inserted that will remain in place for at least seven days, so will also be there when you are at home. Damage to the bowel is very rare.
- Inability to completely empty the bladder (urinary retention). After the operation, it may be that the bladder cannot empty itself, sufficiently. If this happens, a bladder catheter will be reinserted, sometimes for a longer period of time. Usually, the bladder will fully recover.
- Bladder infection (cystitis). The bladder catheter used during the procedure, in some instances, may cause a bladder infection. If you suspect you have a bladder infection, contact your treating physician or your general practitioner.
- Incomplete healing of vagina top. The wound edges at the vaginal apex may become separated, creating an opening between the vagina and the abdominal cavity. Correcting this situation will always require surgery.


Sexuality
It is recommended that you avoid sexual intercourse and the use of tampons for the first six weeks after surgery. There is, however, nothing against becoming sexually aroused or masturbating.
For some people, sexual experience changes after removal of the uterus. Sometimes, these changes are positive, such as having less pain during intercourse. But, in other cases, there are negative changes, such as less interest in intimacy, decreased sensitivity in the area around the vagina or changes in orgasm (coming).
This text was edited on 8-4-2025
Next Step
We recommend that you go through all the information step by step to get a complete picture of the different treatment options and the process around them!

Back to overview

Colpectomy (removal of the vagina)
Colpectomy is a gynecological surgery in which the vagina is removed. Here you can read all about the surgery and the recovery process.
