Phalloplasty
What does phalloplasty involve? How to prepare and what to expect after the operation? Below, you can read about the procedure, the risks involved in the operation, the period after the operation and any subsequent, corrective operations (i.e. secondary corrections). The animations will give you more insight into the operation procedure itself.

About the phalloplasty
The operation
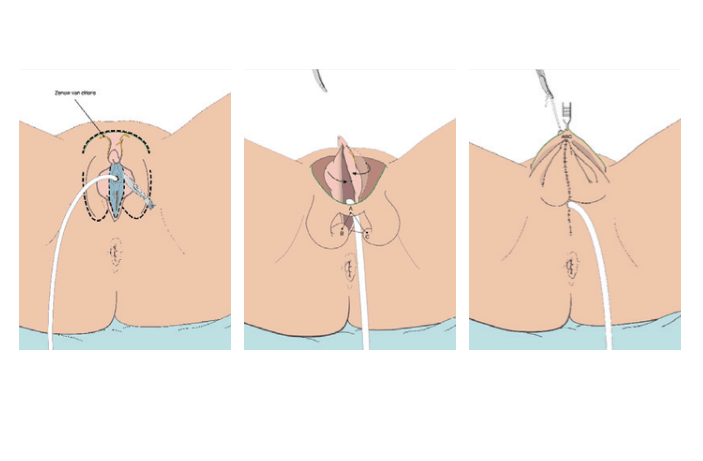
Creating the scrotum

Follow-up and operation techniques
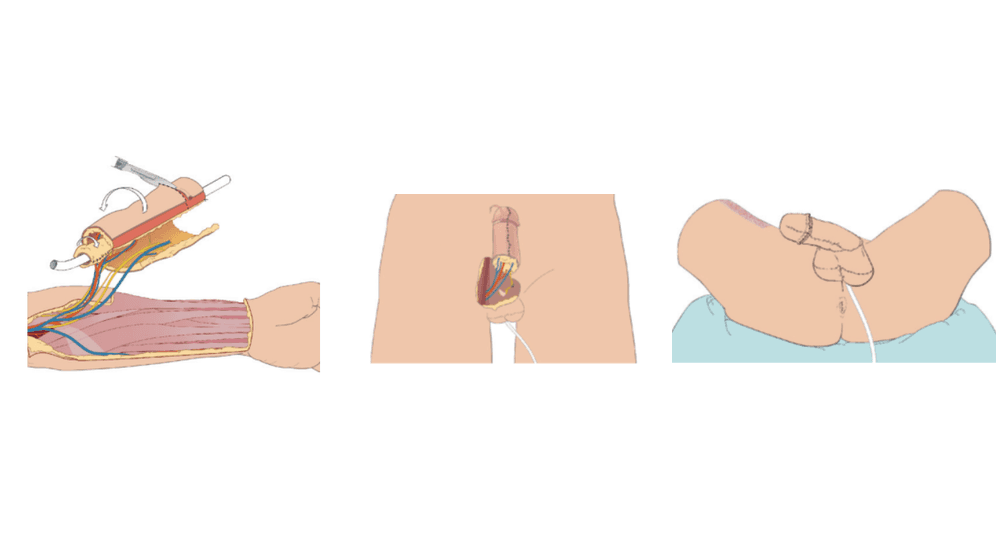
- Phalloplasty without urethral extension – donor skin from the forearm (FRFF)
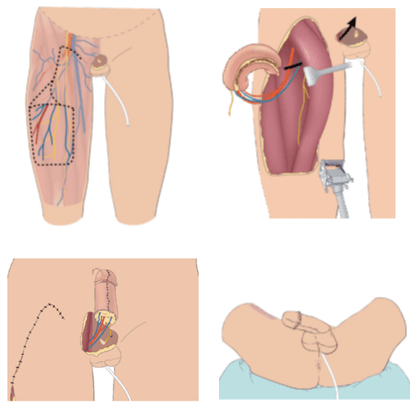
- Phalloplasty without urethral extension – donor skin from the upper leg (ALT)
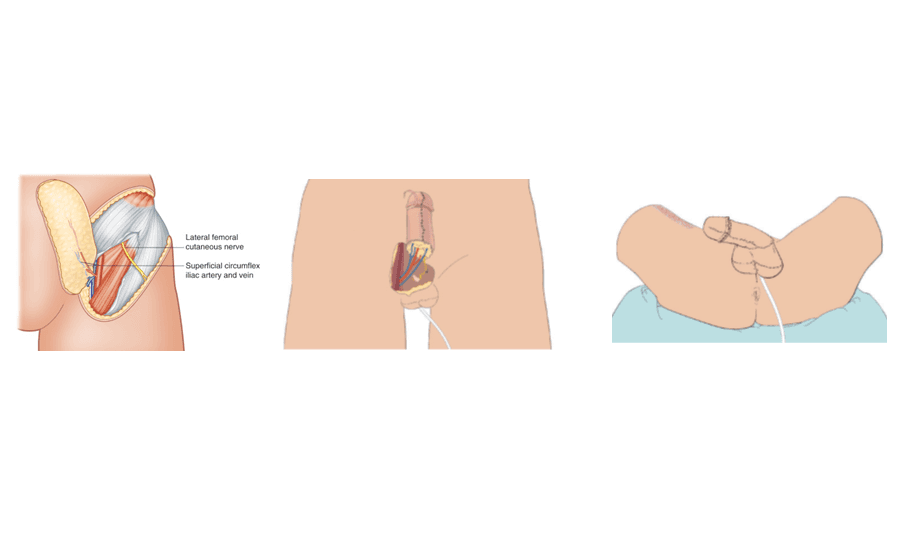
- Phalloplasty without urethral extension – donor skin from the flank (SCIP)
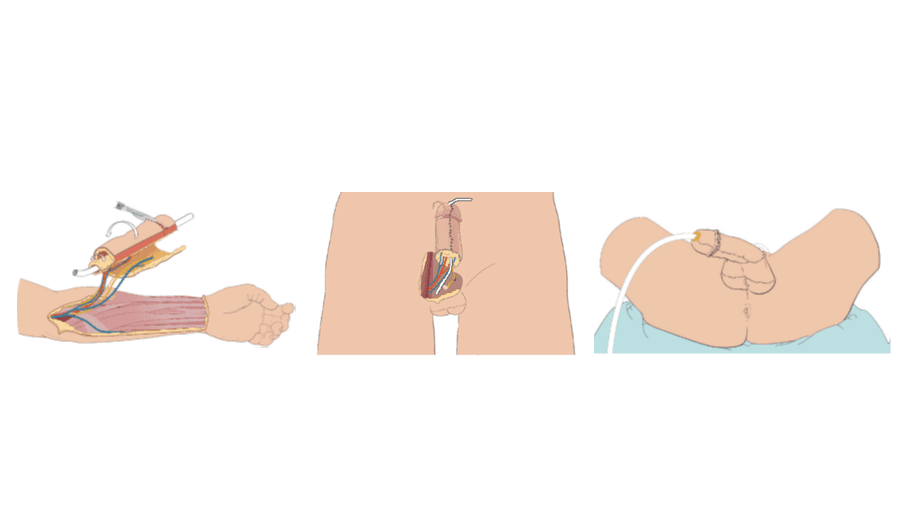
- Phalloplasty with urethral extension – donor skin from the forearm (urethra and shaft)
- Phalloplasty with urethral extension – donor skin from the upper leg (shaft) and the forearm (urethra)
- Phalloplasty with urethral extension – donor skin from the flank (shaft), multiple options for the urethra
1. Phalloplasty without urethral extension — donor skin from the forearm (FRFF)
Scars
2. Phalloplasty without urethral extension — donor skin from the upper leg (ALT)
Scars

3. Phalloplasty without urethral extension — donor skin from the flank (SCIP)
Scars
4. Phalloplasty with urethral extension — donor skin from the forearm
Scars
- Phalloplasty with urethral extension — donor skin from the upper leg (shaft) and forearm (urethra)
Scars

6. Phalloplasty with urethral extension — donor skin from, amongst other things, the flank (shaft)
Scars
Aftercare
Complications and risks during and after the operation
- Haemorrhage. This usually occurs immediately after the operation. Depending on the severity of the bleeding, a second operation may be necessary to stop it.
- Wounds opening up again. Wounds may open, for example, because sutures come apart prematurely. You must take good care of your wounds, as re-suturing is not possible.
- Wound dehiscence (badly healing wounds). Particularly around the sutures, wound healing can become impaired. This often happens to smokers, but sometimes also to non-smokers. This type of wound will generally heal by itself, but it can take a long time. Rinse the wounds regularly with lukewarm tap water and pat the area dry.
- Necrosis (dying tissue). If there is insufficient perfusion in part or all of the skin, tissue will die off. Smokers have an increased risk of this type of complication. Sometimes, this can already be observed during the operation, in which case the surgeon will improve the circulation. In some cases, this occurs not until after the operation. It will usually heal by itself, but sometimes another operation is required.
- Infection. Although the procedure is done in a clean and sterile way, there is always a chance of bacteria entering the wound . This can also happen later, once you are at home. Therefore, it is important that you take good care of your wounds. If the skin around the wound becomes warm and red, if the wound starts to fester or if you get a fever, this may be an indication of the wound being infected and you should contact the plastic surgeon.
- Urination problems (narrowing of the urethra). Narrowing of the urethra (stenosis) may make it difficult to urinate. Stenoses are treated by regularly stretching the urethra, over a number of weeks or months, which is done at the outpatient clinic or by yourself. Sometimes, surgery will be required. The risk of stenosis in cases without urethral extension is 5%, whereas with urethral extension, this is more than 50%.
- Urination problems (fistula). The extended urethra may find an opening to the outside, causing urine to leak out of this opening. This is called a fistula. Sometimes, the opening will heal on its own, but it can also require surgery to correct this situation. Without urethral extension, the risk of a fistula is 5%, whereas with such an extension, this risk is over 50%.
- Urination problems (leakage). Even after a successful urethral extension, leakage is common. The outpatient clinic can provide information and give you instructions on how to massage the urine out of the urethra.
- Loss of feeling/orgasm. Whether you will have feeling in the entire phallus cannot be guaranteed. Both the nerve from the skin and from the former clitoris will need to regrow after the surgery. This process will take anything from months to years and is difficult to predict. Important factors here are your age and smoking behaviour. Your clitoris will be positioned deeper under the skin, which may mean that it will be more difficult or even impossible for you to have an orgasm. However, this complication occurs relatively seldomly.

End result and secondary corrections
End result
Secondary corrections
Prosthetics
Sexuality
Familiarising yourself
This text was edited on 14-10-2022
Next Step
We recommend that you go through all the information step by step to get a complete picture of the different treatment options and the process around them!

Back to overview

Prosthetics after genital surgery
After genital surgery for masculinisation, prosthetics can be placed. Prosthetic testicles are possible after metoidioplasty and phalloplasty. Erectile devices are possible after phalloplasty.
